
Latest episode
1. Psychological Safety is Foundational in Healthcare
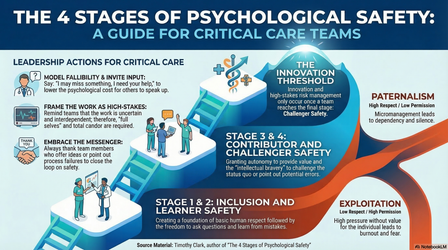
21:27||Ep. 1The Four Stages of Psychological Safety: A Roadmap to Clinical ExcellenceOur focus for this Culture Coalition is psychological safety and its one of the most important requirements for success in healthcare According to Timothy R. Clark, psychological safety is a sequential social exchange. To cross the Innovation Threshold, teams must move through:Inclusion Safety: Inclusion in exchange for human status. Every person in the OR, from the surgeon to the environmental services tech, must feel they belong by right.Learner Safety: Encouragement in exchange for engagement. This allows a resident to ask a "basic" question about a fetal heart rate strip without the psychological cost of embarrassment.Contributor Safety: Autonomy with guidance in exchange for results. This empowers a surgical tech to use their judgment during a complex debulking surgery, applying their skills within clinical guardrails.Challenger Safety: Cover in exchange for candor. This is where a junior nurse feels safe to challenge a senior attending’s decision to induce, prioritizing the patient over the hierarchy. "Challenger safety represents a social exchange of cover in exchange for candor. It is the mechanism that allows for creative abrasion and constructive dissent." Avoiding the "Gutters": Paternalism and ExploitationWhen respect and permission are imbalanced, teams fall into the "gutters."Paternalism (micromanagement) grants respect but denies autonomy, leaving clinicians feeling powerless.Exploitation extracts value while failing to value the human.In these environments, fear becomes a dominant force. Fear is a sign of leadership weakness; it forces clinicians to redirect their energy away from patient care and toward self-preservation, pain avoidance, and personal risk management. Leadership in Action: Framing, Fallibility, and MessengersTo build a safe culture, leaders must adopt three behaviors identified by the Institute for Healthcare Improvement:Framing the Work: Define the work as "uncertain and interdependent." Remind the team that in healthcare, lives depend on our collective vigilance.Modeling Fallibility: Lower the cost of speaking up by admitting your own limits: "I may miss something; I need your eyes on this."Embracing Messengers: You must thank those who offer ideas or point out failures. If you fail to "close the loop" with gratitude, the behavior of candor will die out over time. Conclusion: Why This Matters for InovaFor healthcare, psychological safety is the "lubricating oil" that prevents our clinical habits from becoming fossilized. When we internally compete, we lose our ability to protect our patients; when we connect as partners, we synergize and force multiply our impact.
More episodes
View all episodes

2. Humility is the New Smart
20:41||Ep. 2The Humility Paradox: Surmounting the Smart Machine Age TsunamiIn an era of AI-driven diagnostics, can a world-class surgeon remain relevant when machines process data faster than the human brain? We face a "technology tsunami." Oxford and McKinsey research warns that 45–47% of human tasks are facing displacement. To survive the Smart Machine Age, our teams must pivot. It is no longer about speed or memory—it is about mastering what machines cannot: higher-order critical thinking and deep emotional connection. "Old Smart" is the New Stupid Historically, being smart was a quantity game: memorizing facts and avoiding mistakes. However, machines now possess superior memory, retrieval, and processing speeds. In the SMA, "good is no longer enough." Human competitive advantage has shifted from knowing answers to the quality of our thinking, listening, and collaborating. Humility as a Cognitive Tool In this era, humility is "self-accuracy" and being data-driven, not meekness. It requires "quieting the ego" to become an "open system.""Old smart is the new stupid."We must update our "mental models"—the internal stories we tell ourselves—by decoupling our beliefs from our ego. While we must keep our values, our beliefs must be treated as hypotheses to be constantly stress-tested against new data. The Power of "Otherness" We cannot overcome confirmation bias alone. "Otherness" involves connecting with others to mitigate ego and fear. We need diverse perspectives to challenge our thinking; solo efforts cannot reach the highest levels of innovation or critical thought required to complement machines. The Forward-Looking Conclusion The "myth of Mr. Spock" is dead. Future-of-work excellence demands high emotional engagement and psychological safety. As technology handles routine tasks, businesses must become radically people-centric. Are you ready to quiet your ego and upgrade your mental models to stay relevant?
3. Leaders Eat Last
23:06||Ep. 3Why Healthcare Leaders Must "Eat Last": 3 Biological Truths for Modern Patient CareIn the high-stakes theater of modern medicine, the primary threat to patient safety isn't just clinical error—it’s the biological collapse of the team. Distilled from Simon Sinek’s Leaders Eat Last, the Culture Coalition recognizes that for physicians and nurse leaders, leadership is not a rank; it is a biological responsibility to provide safety. If your staff doesn’t feel safe, they cannot heal. The Biology of the "Circle of Safety": In high-stress clinical environments, trust is a survival mechanism. When a unit lacks a "Circle of Safety," the stress hormone Cortisol "drip-drips" into the system, triggering a survival mode that shuts down the immune system and empathy. This creates "Empathy Fatigue"—a neurological withdrawal where clinicians see patients as tasks rather than people. Conversely, a safe environment fosters Oxytocin, the chemical of trust. As Sinek observed of elite teams, they pull together for one reason: "Because they would have done it for me." Your Job Might Be Killing Your Team (Literally): Chronic cortisol exposure is a physical toxin, contributing to the epidemic of clinician burnout. Many leaders mistakenly chase "performance-based" Dopamine hits—RVU targets or metric bonuses. But Dopamine is highly addictive and dangerous when unbalanced; it rewards the result while sacrificing the human. True fulfillment requires Serotonin, the "Leadership Chemical." It rewards the bond of pride and status between the caregiver and the leader who supports them. Leaders cannot control the complexity of a patient's pathology (the constant), but they are 100% responsible for the internal safety of the unit (the variable). Leadership is a Sacrifice, Not a Perk: Anthropologically, the "Alpha" is granted first choice of meat only because the tribe expects them to run toward danger first. The team voluntarily grants you perks in exchange for protection. Consider the Spartan Shield. A warrior was punished for losing his shield, not his spear. The spear is for individual skill, but the shield is for the person to your left and right. Your value is the protection you offer, not your individual clinical talent. Combatting the "Abstraction" of Care: "Abstraction"—viewing colleagues or patients as data points—is the enemy of clinical empathy. Marine General Flynn famously noted that "Officers Eat Last." This is a literal rejection of abstraction. Email is "easy" but builds zero trust. To trigger oxytocin and restore the human connection, choose the "heavy" energy of the 30-foot walk or a phone call over a digital reply. A Decision, Not a Title: Leadership is a daily choice to look after the person next to you. If the "economy" of your unit shook today, would your team feel safe enough to keep their shields up for one another?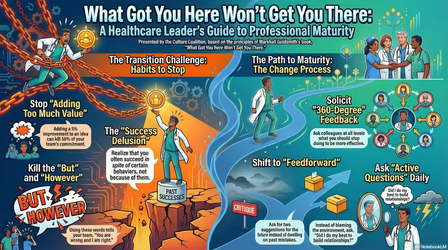
4. What Got You Here Won't Get You There
21:09||Ep. 4Why Your Bedside Success Might Be Blocking Your Leadership PathMany elite clinicians hit a "clinical hero’s ceiling" when transitioning into organizational leadership. The diagnostic reflex that saves lives at the bedside often becomes a liability in the boardroom. These insights, discussed within the Culture Coalition, draw from the core principles of Marshall Goldsmith’s What Got You Here Won’t Get You There. Bedside excellence is about individual performance; leadership is about enabling the achievement of the entire multidisciplinary team.The Trap of "Winning Too Much" Medical training rewards being right, but leadership requires "relational capital." Clinicians often burn this capital by winning trivial battles—like arguing over a non-clinical scheduling preference or the specific layout of a supply room. In leadership, winning a minor point at the expense of team rapport is a net loss for organizational cohesion and long-term results.When "Adding Value" Kills Commitment The impulse to "fix" every plan is a hallmark of the high-achiever who subconsciously believes they are the smartest person in the room. When you "improve" a nurse's or junior MD's idea by adding your "two cents," you are essentially telling the world how smart you are at the expense of their ownership. Goldsmith captures the danger perfectly:"The quality of the idea may or may not go up 5% but my commitment just went down 50%."Acknowledging an idea without modification is a more powerful move because it preserves the team's drive to execute the plan.The Power of the "Stop" List Peter Drucker noted that leaders should focus on what to stop doing. For busy MDs and RN leaders, stopping a behavior is more efficient than learning a new one. Relevant "bad habits" to eliminate include:Passing Judgment: Grading every idea creates a fearful, pressurized culture.Starting with "No," "But," or "However": These qualifiers signal "I’m right, you’re wrong."Failing to Give Recognition: Withholding praise depletes motivation and sows resentment.Telling the World How Smart We Are: Displaying intellectual superiority creates a barrier to authentic partnership.Moving from Feedback to "Feedforward" Clinicians are often sensitized to "feedback" because it traditionally follows a clinical error or "near miss." Unlike past-oriented feedback, "feedforward" carries no baggage. It focuses on a positive future through a four-step dialogue: Pick a behavior to change, describe the objective, ask for future-oriented suggestions, and listen without judgment—simply saying "Thank you."The Mirror and the Mission Professional maturity requires evolving from a "doer" to a partner in the mission. If your team’s success is the new metric of your own, what is the one behavior you are willing to stop today to help them get there?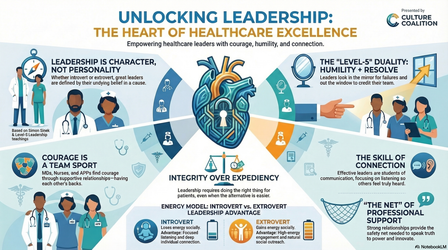
5. The Architecture of Level-Five Leadership
21:15||Ep. 5Why the Best Healthcare Leaders Aren’t Who You Think They AreA New Paradigm for the Hospital Floor We have long misdiagnosed leadership in clinical settings. The pervasive myth that an effective leader must possess "bounce-off-the-walls" charisma often sidelines our most capable clinicians. Drawing on the work of the Culture Coalition and author Simon Sinek, we are seeing a shift: the most impactful physician, nurse, and APP leaders aren't necessarily the loudest—they are the ones who prioritize psychological safety and unwavering purpose. To build resilient teams, we must unlock leadership at all levels, recognizing that traditional extroversion is not a prerequisite for command.Introversion as a Strategic Resource Sinek clarifies that introversion is not social awkwardness; indeed, many extroverts are socially inept. Rather, it is a matter of energy. Using the "coin" analogy, an introvert spends energy on social interactions, while an extrovert gains it. For the clinician who finds a busy shift depleting, this is a strategic resource, not a deficit. Introverts excel by leveraging one-on-one connections. Instead of "holding court," they provide individuals with a "whole idea" or a "whole thought," building deep trust during rounds or huddles."The one thing [leaders] all have to have in common... is undying belief in your cause... charisma is how much you're willing to devote to that and if it's all of it you have charisma you have leadership capacity."Courage is a Team Sport We mistakenly view courage as an internal fortitude. Sinek argues it is actually external—functioning like a trapeze artist’s net. In healthcare, that "net" is the quality of your relationships. Investing in the person to your left and right provides the energy needed to speak truth to power, report a safety concern, or do the right thing under overwhelming pressure. Courage is the result of knowing someone has your back if things go sideways.The "Level 5" Duality: Resolve and Humility Research identifies "Level Five Leadership" as a rare blend of fierce professional resolve and personal humility. These leaders use the "Mirror and the Window" metaphor: they look in the mirror to accept blame for setbacks and out the window to credit their team for success. This humility is not a lack of drive; it is the redirection of ambition away from the ego and toward the mission.Beyond the Law of Expediency Management often follows the "law of expediency"—doing what is fast or merely legal. True leadership demands integrity, a much higher standard. As you lead your unit, consider: Who is the "net" that gives you the courage to do what is right, and whose net are you?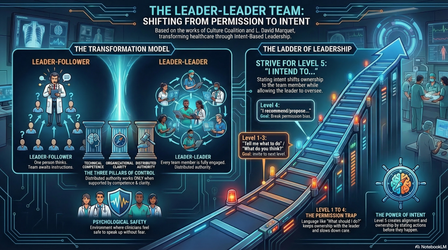
6. Intentional Leadership - Moving from a Leader-Follower to a Leader-Leader Model
21:24||Ep. 6From Submarines to Healthcare: Why Your Hospital Team Needs a 'Leader-Leader' RevolutionIn high-acuity clinical environments, the "Industrial Era" model of scientific management is a strategic liability. Hospitals often treat clinicians like assembly-line workers in a "Leader-Follower" structure—a relic designed for repetitive physical labor, not the complex knowledge work of modern medicine. This top-down control creates organizational fragility and "learned helplessness." To achieve excellence, healthcare must adopt the "Leader-Leader" revolution pioneered by retired Navy Captain David Marquet in Turn the Ship Around! and Leadership is Language.The Power of "I Intend To" Traditional organizations are permission-based, where staff wait for a stamp of approval, creating dangerous clinical bottlenecks. Marquet’s "Intent-Based" model shifts language to "I intend to..." This moves the "psychological oxygen" to the bedside where the information lives. Crucially, it flips the bias to action: the team proceeds unless the leader exercises a veto."Requiring a fuller explanation had the added benefit of pushing them to think at a higher level. This was, in effect, a leadership development program."By stating intent, clinicians take ownership of outcomes rather than just following orders.Strive for Five: The Ladder of Leadership The "Ladder of Leadership" provides a roadmap to move staff from Level 1 ("Tell me what to do") to Level 5 ("I intend to"). Leaders invite the team higher by asking intermediate, rung-climbing questions: What do you see? What do you think? What do you recommend?Strive for Five. Level 5 is the sweet spot for collaboration because intent is stated before the action occurs, allowing for input without the delay of a permission request. Conversely, moving to Levels 6 and 7 ("I did...") reduces safety by removing the opportunity for collaborative oversight.Combatting "Clinical Autopilot" with Deliberate Action When clinicians are told to "just follow orders," their brains are rewired for passivity. To break this "clinical autopilot," we must implement Deliberate Action. This mechanism requires a clinician to Pause, Verbally State Intent, and Gesture (e.g., pointing at the medication vial or monitor). This physical act engages the prefrontal cortex, forcing the brain from mindless execution to conscious expertise.Conclusion: Beyond Compliance to Excellence Strategic leadership is not about "avoiding errors" through compliance; it is about "achieving excellence" through distributed authority. As you walk onto your unit today, ask yourself: Are you building followers who wait for orders, or leaders who own the outcome?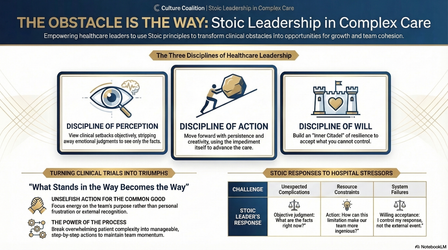
7. The Obstacle is the Way
20:54||Ep. 7The Patient is the Path: Stoic Strategy for the Modern ClinicManaging a clinical unit is a gauntlet of noise—unpredictable decompensations, staffing gaps, and emotional fatigue. The Culture Coalition recently examined how ancient wisdom serves as a high-stakes leadership framework for navigating this chaos. Drawing from Marcus Aurelius’s Meditations and Ryan Holiday’s The Obstacle Is The Way, we propose a shift in perspective: For MDs, RNs, and APPs, obstacles are not interruptions to the work; they are the work. Consider every setback as "medicine" prescribed by nature—bitter, perhaps, but necessary for the organization’s healing and growth.Discipline of Perception: Deconstruct the DisasterStoicism centers on Logos—the rational laws connecting the universe. In clinical chaos, your task is to strip away the "narrative of disaster" and see only the facts. Maintain "nerve control" by deconstructing the crisis into its smallest parts. Just as a musician masters a song note by note, or a dancer studies a single motion, analyze the individual elements of a code or a discharge delay. When you isolate the smallest moment, you realize it has no power over you. Facts allow for logic; narratives fuel panic.Discipline of Action: Follow the ProcessIgnore the distant goal of the cure or the discharge. Focus exclusively on the immediate task in front of you. Thomas Edison iterated through 6,000 filaments to find one that worked; clinical leadership requires that same relentless iteration through failing protocols without emotional exhaustion. Command your attention to the next seven seconds, the next order, or the next patient interaction. Well-being is realized by small, deliberate steps."The impediment to action advances action. What stands in the way becomes the way." — Marcus AureliusDiscipline of Will: Unity Over SelfTrue resilience is rooted in Amor Fati—the love of fate. Accept what lies outside your control: physiology, resource shortages, and human error. Use these constraints as fuel for your character. Admiral James Stockdale used the acronym "U.S.": Unity Over Self. As "higher creatures," we exist to support the community. When you stop fighting reality and embrace your duty to the team, you find a source of motivation that external stressors cannot touch.A New Standard of LeadershipClinical excellence is the mastery of obstacles, not their absence. Refine your perception, command your actions, and steady your will. Mastery is not a destination, but a way of moving through the clinic.The Rounding Reflection: During your next shift, ask: "Am I reacting to a narrative of disaster, or am I seeing the facts as they truly are?"